Reconstruction of mastectomy defects is challenging. It is even more challenging in the face of radiation. Not all tissues and tissue types tolerate radiation to the same degree. In some patients implant reconstructions are not amenable after they have undergone radiation. Improving the tissue characteristics is important to making an implant reconstruction a viable option.
One of the more common indications for a latissimus dorsi reconstruction is a patient who has undergone radiation therapy after mastectomy and who has had challenges with attempts at implant reconstruction. Patients who have prior abdominal scars or who do not have usable abdominal tissue are often patients who undergo latissimus dorsi flap reconstruction.
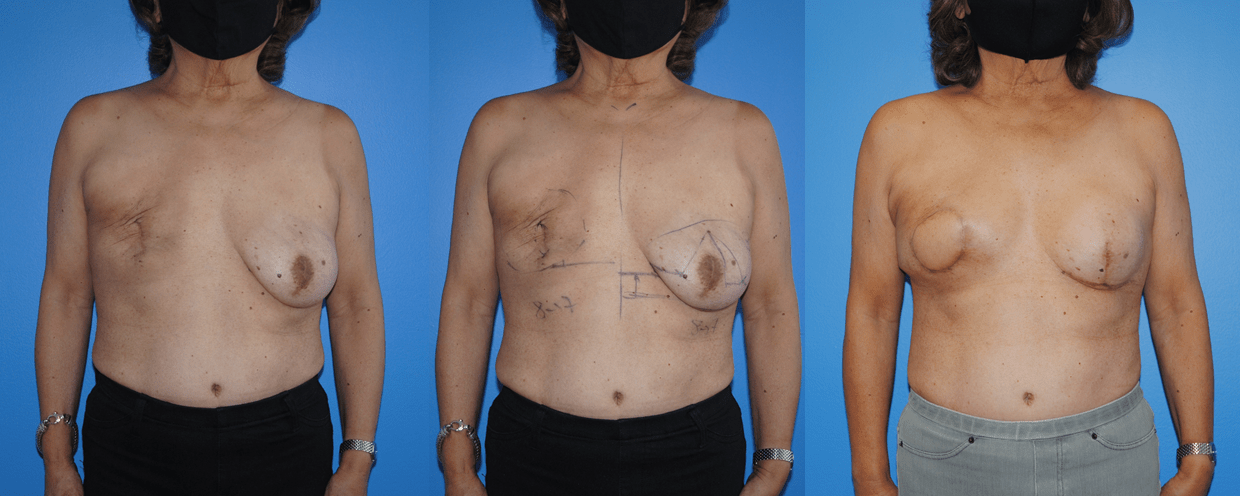
Often the radiated breast has a tight skin envelope with an elevated infra-mammary fold. Trying to reconstruct a breast with ptosis on this side is challenging without ample abdominal tissue. The best option for symmetry is to perform a mastopexy or breast lift on the contralateral breast. In this case the patients left side had already undergone a mastectomy and the nipple areola complex can not be elevated. Matching position of nipple areola complexes, would best be accomplished with nipple areola complex tattoo once the reconstruction is complete.
The last photograph in the series shows a tissue expander beneath a latissimus dorsi myocutaneous flap. The tissue expander and soft tissue construct are allowed to heal and stabilize before final stage revision with removal of the tissue expander and insertion of a soft mammary prosthesis.
The latissimus dorsi donor site can be concealed within the bra-line on the posterior trunk. This can help minimize donor site visibility.
